Biology (SJCR)
Stechnolock Journal of Case Reports
Full Text
Volume 2, Issue 1
Giant Adrenal Cyst: Case Report
*Corresponding Author: Abraham Ariaya, Department of Surgery, St. Paul's Hospital Millennium Medical College, Addis Ababa, Ethiopia, Tel: +251961016194, E-mail: abraham.ariaya@gmail.com
doi: /sjcr.2021.2.105
Citation: Abraham Ariaya, Yishak Suga, Birhanetensay Teklewold, Melat Debebe, Befekadu Limmu, et al (2022) Giant Retroperitoneal Liposarcoma: Case Report. Stechnolock J Case Rep 2: 1-4
Copyright: © 2022 Abraham Ariaya. This is an open-access article distributed under the terms of Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
.JPG)
.JPG)
Abstract
Adrenal cysts are rare cystic masses that arise from the adrenal gland. The cysts are usually small (<10 cm) in size, nonfunctional, unilateral, asymptomatic often seen in females. However adrenal cysts can attain huge sizes surpassing a diameter of 10 cm (Giant) and become symptomatic. When adrenal cysts are Giant, patients present with flank pain. Here, we report a 26 years old female patient who presented with left flank pain of 2 years duration who was later diagnosed to have an18cm x 10cm adrenal cyst which required an adrenal sparing cyst excision.
Keywords: Giant; Adrenal; Cyst; Adrenal Sparing Excision
Introduction
Adrenal cysts are rare occurrences with an incidence of 0.064 - 0.18% at autopsy. They are also reported to have an incidence of 5.4% in clinical series. But the diagnosis of Adrenal cysts is currently on the rise as cases of incidentalomas due to increasing use of diagnostic imaging modalities. [1, 2, 3, 4]
Adrenal cysts are usually small in size and asymptomatic but have been reported with rapid increase in size due to intra-cystic haemorrhage to attain increased sizes. Surgical exploration provides the definitive diagnosis when accompanied with pathology. Surgery is indicated when the cyst size exceeds 10 cm in diameter, in the presence of symptoms, endocrine abnormalities, intra-cystic bleeding and suspicion of malignancy. [1] Here, we report a 26 years old female presented with symptomatic giant left adrenal cyst which required an adrenal sparing cyst excision.
Case Report
A 26 years old female patient presented to our hospital with a complaint of left flank dull aching, non-radiating pain of 2 years. She had been given various antibiotics as treatment for presumed urinary tract infections at different times with no improvement.
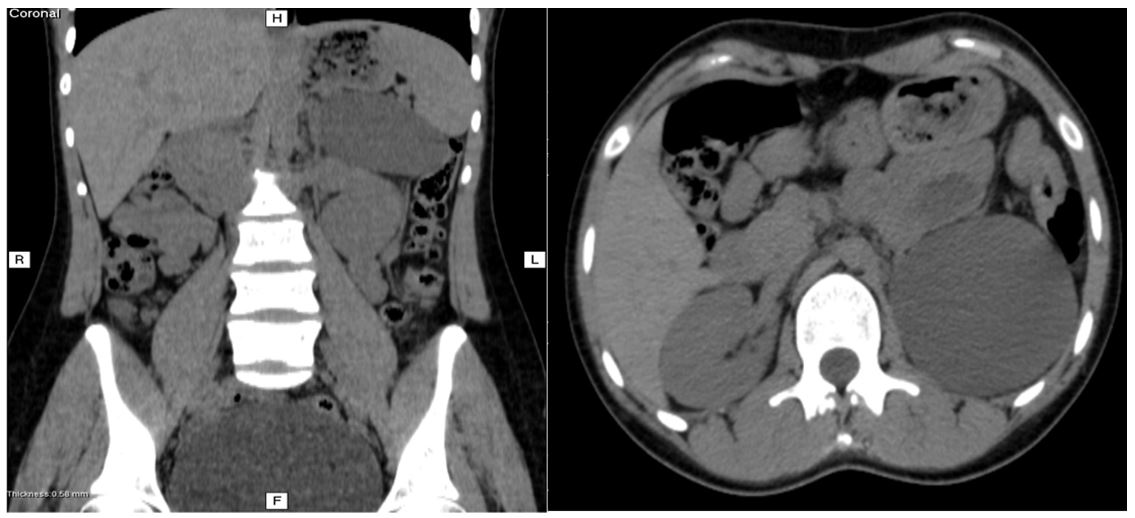
On examination she had normal vital signs and abdominal examination except mild flank tenderness. A full blood work up reveal no abnormality. Her serum cortisol and urinary catecholamine levels were assessed and were within the normal range. Abdominal CT scan showed a large round water attenuating non-enhancing left suprarenal lesion that has no septations. The lesion had displaced the left kidney downwards. Apart from the displacement no abnormality was noted on the kidneys.
She was subsequently operated and an adrenal sparing open cyst excision was done through left subcostal incision. Intra-op finding was approximately 10cm x 18cm x 8cm cyst arising from the left adrenal gland. The cyst was dissected carefully and freed from the kidney, adrenal parenchyma and then cyst excision was completed. There was no intra-op accident except cyst rupture. The patient left the operation theater with stable vital signs and had an uneventful post-operative stay in the wards and discharged on 2nd post-operative day.
The excised specimen was sent for pathology and it revealed a flattened lining and adjacent normal adrenal gland with a diagnosis of an endothelial adrenal cyst.
The patient had subsequent follow ups on her 2nd and 4th post op weeks, her previous flank pain symptoms had subsided and she was able to continue her normal day to day activities.
Discussion
Adrenal cysts have been known since the late 17th century. Greaseless, a Viennese anatomist, first described them in 1670 as the cause of death of a 45 years old nobleman after an adrenal cyst filled with 12 pounds of fluid ruptured. [1, 3, 4].
Adrenal cysts can present as asymptomatic incidentalomas identified on routine sonograms or CT scans requested for other complaints. They can also present with flank pain as in our case and complications such as hypovolemic shock due to the rapidly increasing haemorrhage into the cysts causing an increase in diameter of the cyst. While most adrenal cysts are smaller than 10 cm in diameter, cysts as large as 45 cm have been reported. [2]
Adrenal cysts are commonly seen in the fourth and fifth decade of life. It, occur in 5.1% of adrenal disease and may be malignant with an incidence of 7% cases. [3, 4, 5]
An institution based study conducted by Xiao Lyu et al. which analysed the surgical management of cystic lesions of the adrenal gland in 47 patients have concluded that 61.7% occurred in females and all cysts were unilateral. The unilateral nature of cysts has been disputed in a study by Daniel et. al. which account for 10% of cases occurring bilaterally. [3, 4] But, Daniel and et als have reported bilateral adrenal cysts in 10% of their serious
Cystic lesions of the adrenal gland have been traditionally classified into four with different studies putting forwards differing incidences, they are namely endothelial cyst, pseudocyst, epithelial cyst and parasitic cyst. Endothelial and pseudocysts have alternatively been put as the most common varieties in several studies [1, 2, 3, 4] Our patient has an endothelial cyst.
With regard to management, both laparoscopic and open procedures are practiced. Both laparoscopic and open approaches have equivalent efficacy with the former providing a shorter hospital stay and better cosmetic results. [3]
In both approaches there is a choice between adrenal sparing cyst resections and adrenalectomies. In our case we preferred the open procedure with an adrenal sparing approach because our experience with laparoscpy is very limited.
Summary
Adrenal cysts are rare occurrences. It would be wise to include them in the list of differential diagnosis of abdominal and flank area symptoms. With the current increased availability of imaging modalities there is an increase in the rate of diagnosis of adrenal cysts. This warrants an understanding into the possible management options after a thorough physical examination.
Competing Interests
The authors declare no competing financial or personal interest
- T Atim et al. (2016) "Giant adrenal cyst in a young female patient: A case report", African Journal of Urology 22: 83-5
- Catalina Poiana et al. (2010) "Giant adrenal cyst: case study," J Med and Life 3: 308‐13
- Xiao Lyu et al. (2014) "Surgical management of adrenal cysts: a single-institution experience," Int Braz J Urol 40: 656-65
- Daniel Paramythiotis et al. (2018) "Surgical Management of a Giant Adrenal Pseudocyst: A Case Report and Review of the Literature in the Last Decade," Case Rep Surg 8473231
- Subbarao Chodisetti et al. (2016) "Giant adrenal cyst displacing the right kidney," Indian J Urol 32: 1.